

Volume 6, Issue 2 (April 2022)
AOH 2022, 6(2): 1230-1235 |
Back to browse issues page


![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Lai A, Trivedi A, Ishak N, Ahmad N, Omar N. COVID-19 Surveillance in Workplaces: a Success Story of Surveillance in Migrant Workers in Brunei Darussalam. AOH 2022; 6 (2) :1230-1235
URL: http://aoh.ssu.ac.ir/article-1-301-en.html
URL: http://aoh.ssu.ac.ir/article-1-301-en.html



1- Occupational Health Division, Ministry of Health, Brunei Darussalam• PAPRSB Institute of Health Sciences, Universiti Brunei Darussalam , ALSC91@HOTMAIL.COM
2- Occupational Health Division, Ministry of Health, Brunei Darussalam
2- Occupational Health Division, Ministry of Health, Brunei Darussalam
Full-Text [PDF 1870 kb]
(201 Downloads)
| Abstract (HTML) (857 Views)
s estimated by International Labor Organization (ILO), 244 million migrants, out of 3.3% of the global population, contribute to the economies of both host and home country.1 COVID-19 pandemic has exposed health inequalities of this vulnerable group between and within countries.2 A recent systematic review highlighted the higher risk of adverse health outcomes as a result of the higher proportions of COVID-19 infection in the migrant worker population. This is because only a small number of SARS-CoV-2 tests were done on them, compared to the native population.3 Other attributes include their overcrowded work and accommodation conditions, language barrier and lack of awareness, and lack of accessibility to health services. All of these are risk factors for widespread transmission of infectious diseases.3 In April-May 2020, the initial outbreak of COVID-19 in countries such as Singapore and Saudi Arabia was driven mainly by local transmission among migrant construction workers. By May 6 2020, Singapore had reported that 88% (17,758) of their total cases were among dormitory migrant workers.4, 5 Similarly, more than 50% of the national cases in Saudi Arabia reported by mid-April 2020 were among their migrant worker population.6 Having observed this experience of other nations, Brunei Darussalam implemented an active and enhanced surveillance strategy early on, to provide free screening and testing for the migrant worker population.7
Brunei Darussalam sits on the island of Borneo in Southeast Asia, with a total population of 459,000, and a total employed workforce of 237,944. Migrant workers make up 74,268 (33.5%) of the workforce.8 Brunei Darussalam reported its first case of COVID-19 on March 9 2020, and by July 31 2021, there were 337 cases recorded. This included 141 cases of local transmission, with the last case reported on May 6 2020, which was followed by 196 imported cases from overseas.9
The Ministry of Health (MOH) adopted an active and enhanced surveillance strategy for SARS-CoV-2, to screen the migrant worker population in the country. The purpose was early detection and breaking the chain of SARS-CoV-2 transmission in the workplace and community.
Methods
Active surveillance of SARS-CoV-2 was carried out on the migrant worker population, in three phases by MOH through the Occupational Health Division, from April 2020 to April 2021. The flowchart of the advanced monitoring strategy for COVID-19 in the migrant worker population in
Brunei Darussalam is shown in Figure 1.
Nasopharyngeal swab for reverse transcriptase polymerase chain reaction (RT PCR) was used to test for SARS-CoV-2 in phases I and II, whilst rapid antigen test was used during phase III of the surveillance. These tests were offered free of cost and independent of other COVID-19 active surveillances for contact tracing, influenza-like illness, travel related cases and hospital admissions. In all three phases, the process of random selection of migrant workers from registered companies was done through inter-governmental collaboration with the Department of Labor, Ministry of Home Affairs. 10% of the respective company’s migrant workers were randomly selected for screening, via submission of name list through the company's human resources personnel.
Results
Figure 2 shows the step-by-step approach to active COVID-19 monitoring of the migrant worker population in Brunei Darussalam. Phase I was conducted from April 7, 2020 to June 27, 2020. Workers were selected by a two-stage sampling method: the first stage involved purposive selection of 714 companies, prioritized in view of their higher risk of exposure. This was because these workplaces had public facing or client serving activities; the second stage was a random selection of 10% of the migrant workforce from each of the identified workplaces for RT PCR testing.
Most of the migrant workers who were screened and tested were men (87.9%), and aged between 20-40 (62.8%). Migrants from various nationalities were tested, with the top five nationalities being Indonesia (33.5%), Bangladesh (19.5), the Philippines (17.4), Malaysia (12.0%) and India (11.8%).

Figure 2. Phased approach for COVID-19 active surveillance in the migrant worker population in Brunei Darussalam
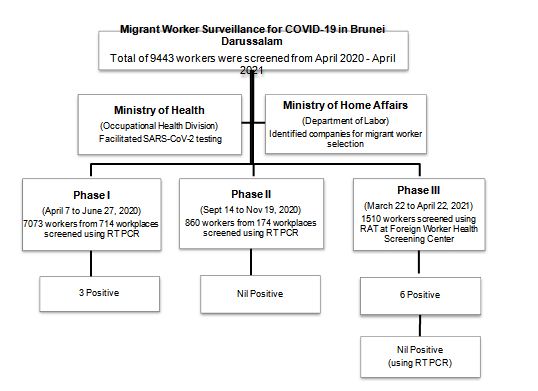
Figure 1. Flowchart of enhanced surveillance strategy for COVID-19 in the migrant worker population in Brunei Darussalam
Full-Text: (252 Views)
COVID-19 Surveillance in Workplaces: a Success Story of Surveillance in Migrant Workers in Brunei Darussalam
Alice Lai 1,2*, Ashish Trivedi 1, Norzawani Ishak 1, Norzalena Ahmad 1, Nurasiah Omar 1
1 Occupational Health Division, Ministry of Health, Brunei Darussalam• 2 PAPRSB Institute of Health Sciences, Universiti Brunei Darussalam• *Corresponding authors: Alice Lai, Email: alice.lai@moh.gov.bn
ABSTRACT
Background: Migrant workers are at a high risk of exposure to COVID-19 due to their work and residential status. Surveillance for SARS-COV-2 in this group is important for early detection of infection and breaking the chain of disease transmission in the workplace and community. This report describes an enhanced active surveillance strategy for COVID-19 in migrant workers of Brunei Darussalam during the first wave of the outbreak in 2020. Methods: Active and phased surveillance of migrant workers for SARS-CoV-2 was conducted by the Ministry of Health on a total of 9443 workers, in 2020. Surveillance was carried out using a nasopharyngeal swab test for SARS-CoV-2 reverse transcription-polymerase chain reaction (RT PCR) in phases I and II, whilst a rapid antigen test was used in phase III. Results: Phase I included 7073 workers from 714 workplaces; phase II covered 860 workers from 190 workplaces; and phase III covered 1510 workers. Three positive cases were detected during phase I of the surveillance. No migrant worker was tested positive for SARS-CoV-2 during the second and third phases of surveillance. Conclusion: The number of positive cases detected was small; however, this strategy actively searched for the presence of SARS-CoV-2 among the migrant worker population in the country, and further confirmed the absence of any hidden local transmission of cases in this population.
Keywords: Migrant Worker; COVID-19; Surveillance; Screening; Workplaces
Introduction
Alice Lai 1,2*, Ashish Trivedi 1, Norzawani Ishak 1, Norzalena Ahmad 1, Nurasiah Omar 1
1 Occupational Health Division, Ministry of Health, Brunei Darussalam• 2 PAPRSB Institute of Health Sciences, Universiti Brunei Darussalam• *Corresponding authors: Alice Lai, Email: alice.lai@moh.gov.bn
ABSTRACT
Background: Migrant workers are at a high risk of exposure to COVID-19 due to their work and residential status. Surveillance for SARS-COV-2 in this group is important for early detection of infection and breaking the chain of disease transmission in the workplace and community. This report describes an enhanced active surveillance strategy for COVID-19 in migrant workers of Brunei Darussalam during the first wave of the outbreak in 2020. Methods: Active and phased surveillance of migrant workers for SARS-CoV-2 was conducted by the Ministry of Health on a total of 9443 workers, in 2020. Surveillance was carried out using a nasopharyngeal swab test for SARS-CoV-2 reverse transcription-polymerase chain reaction (RT PCR) in phases I and II, whilst a rapid antigen test was used in phase III. Results: Phase I included 7073 workers from 714 workplaces; phase II covered 860 workers from 190 workplaces; and phase III covered 1510 workers. Three positive cases were detected during phase I of the surveillance. No migrant worker was tested positive for SARS-CoV-2 during the second and third phases of surveillance. Conclusion: The number of positive cases detected was small; however, this strategy actively searched for the presence of SARS-CoV-2 among the migrant worker population in the country, and further confirmed the absence of any hidden local transmission of cases in this population.
Keywords: Migrant Worker; COVID-19; Surveillance; Screening; Workplaces
Introduction
| A |
Brunei Darussalam sits on the island of Borneo in Southeast Asia, with a total population of 459,000, and a total employed workforce of 237,944. Migrant workers make up 74,268 (33.5%) of the workforce.8 Brunei Darussalam reported its first case of COVID-19 on March 9 2020, and by July 31 2021, there were 337 cases recorded. This included 141 cases of local transmission, with the last case reported on May 6 2020, which was followed by 196 imported cases from overseas.9
The Ministry of Health (MOH) adopted an active and enhanced surveillance strategy for SARS-CoV-2, to screen the migrant worker population in the country. The purpose was early detection and breaking the chain of SARS-CoV-2 transmission in the workplace and community.
Methods
Active surveillance of SARS-CoV-2 was carried out on the migrant worker population, in three phases by MOH through the Occupational Health Division, from April 2020 to April 2021. The flowchart of the advanced monitoring strategy for COVID-19 in the migrant worker population in
Brunei Darussalam is shown in Figure 1.
Nasopharyngeal swab for reverse transcriptase polymerase chain reaction (RT PCR) was used to test for SARS-CoV-2 in phases I and II, whilst rapid antigen test was used during phase III of the surveillance. These tests were offered free of cost and independent of other COVID-19 active surveillances for contact tracing, influenza-like illness, travel related cases and hospital admissions. In all three phases, the process of random selection of migrant workers from registered companies was done through inter-governmental collaboration with the Department of Labor, Ministry of Home Affairs. 10% of the respective company’s migrant workers were randomly selected for screening, via submission of name list through the company's human resources personnel.
Results
Figure 2 shows the step-by-step approach to active COVID-19 monitoring of the migrant worker population in Brunei Darussalam. Phase I was conducted from April 7, 2020 to June 27, 2020. Workers were selected by a two-stage sampling method: the first stage involved purposive selection of 714 companies, prioritized in view of their higher risk of exposure. This was because these workplaces had public facing or client serving activities; the second stage was a random selection of 10% of the migrant workforce from each of the identified workplaces for RT PCR testing.
Most of the migrant workers who were screened and tested were men (87.9%), and aged between 20-40 (62.8%). Migrants from various nationalities were tested, with the top five nationalities being Indonesia (33.5%), Bangladesh (19.5), the Philippines (17.4), Malaysia (12.0%) and India (11.8%).
Figure 2. Phased approach for COVID-19 active surveillance in the migrant worker population in Brunei Darussalam
Figure 1. Flowchart of enhanced surveillance strategy for COVID-19 in the migrant worker population in Brunei Darussalam
Results were communicated to the workers through their company's human resources focal point. During phase I of surveillance, a total of 7073 migrant workers were tested, out of whom three tested positive for RT PCR. Following the national standard operating procedure, positive cases were taken to the National Isolation Centre, and later, they recovered uneventfully. All three workers were from the same workplace, and shared the same residential accommodation. Contact tracing was done at their workplace and residence for close contacts, sent for RT PCR test, and all were tested negative.
Phase II was conducted from September 14, 2021 to November 19, 2021. By then, there were no local transmission cases, and positive cases were limited to only imported cases who had travelled into Brunei Darussalam from overseas. During this phase, a total of 190 companies were identified, and 10% of each company’s migrant workforce was selected for RT PCR testing. Out of 174 companies, 860 migrant workers were screened and tested negative. By then, Brunei had recorded 197 days of zero COVID-19 in local cases, and this may have been the probable reason for suboptimal participation of companies and migrant workers during this phase of active surveillance.
A different approach was adopted for phase III, which was conducted from March 22, 2021 to April 22, 2021. At this point, MOH had acquired a supply of COVID-19 antigen rapid test kits. This point of care testing was conducted at the Foreign Worker Health Screening Center, where migrant workers attended for their biennial health screening as part of their employment visa process.10 Every 5th migrant worker who attended the center was selected, which resulted in a total of 1510 migrant workers. Most of them were 30-40 years of age (35.8%) and men (68.3%). A similar distribution of the above nationalities was observed in this cohort; namely Indonesia (39.7%), Philippines (27%), Bangladesh (12%) and India (10.4%). Six of the workers were tested positive for SARS-CoV-2 antigen; however, according to the confirmatory RT PCR test done on the same day, all six results turned out to be negative.
Discussion
As SARS-CoV-2 does not discriminate against any individual, the migrant worker population is not spared from the virus. Their risk is often increased due to overcrowded living conditions, lack of accessibility to healthcare and hygiene practices, language and socio-cultural barriers.11,12 The World Health Organization (WHO) had published several guidance documents on COVID-19 surveillance in high risk populations. They included site-specific risk assessment and community-based surveillance as important strategies to prevent and contain rapid spread of the virus.11, 12 This paper described an active workplace surveillance for SARS-CoV-2, among migrant workers in Brunei Darussalam in a phased manner during the different stages of COVID-19 outbreak in the country. Phase I (April-June, 2020) of the surveillance was carried out when there was active community transmission, while phases II (September-November 2020) and III (March-April 2021) were conducted when there was no ongoing community transmission. Phase I identified three COVID-19 cases, that ultimately turned out to be the last three reported cases during Brunei’s first wave of outbreak. However, no positive cases were identified during phases II and III, which ensures the absence of any ongoing hidden transmission of disease. This low incidence can be attributed to an overall low level of infection during the first wave of COVID-19 in the country, i.e. a total of 141 cases reported from March 9, 2020 to May 6, 2020. This was followed by 196 imported cases entering Brunei from overseas by July 31, 2021. During the first wave, Brunei also recorded zero COVID-19 cases among healthcare workers, another high risk group identified for SARS-CoV-2 transmission globally.13 This successful control of pandemic was a result of strict public health measures adopted by MOH Brunei. It included restrictions of overseas travel and mass gatherings, increasing awareness and practices on hygiene measures and physical distancing, isolation/quarantine measures, as well as enforcing legislative provisions under the Infectious Disease Act of 2010. A test, trace and isolate approach and regular screening of high risk groups, such as healthcare workers and migrant workers, helped the nation to mitigate the threat of transmission of SARS-CoV-2.14, 15
Conclusion
Active COVID-19 screening of migrant workers in phase I during the time of ongoing community transmission, helped to detect three positive cases. They turned out to be the last reported local cases during the first wave of outbreak. Though the number of positive cases was small, this strategy actively searched for any positive cases among the registered migrant worker population in the country. Phases II and III of surveillance activities, further confirmed the absence of any hidden local transmission case in this population. Thus, a continuous phased and enhanced active surveillance strategy is beneficial not only in detecting local transmission cases that probably would have gone undetected, but also in confirming absence of any hidden ongoing transmission in this population. In addition, such data are useful to inform local authorities to take subsequent actions regarding further containment of COVID-19, and for collaborative efforts to be strengthened between the health sector and other relevant sectors responsible for health, safety and welfare of migrant workers in Brunei Darussalam.
Key Points for Enhanced Surveillance in Migrant Worker Population:
• Identifying high risk or vulnerable populations
• Developing or using an existing surveillance system to facilitate screening and testing in this population
• Collaborating with relevant organizations to facilitate surveillance
• Offering free surveillance screening and testing to migrant worker population
Conflict of Interest
None
Author's contributions
AL conceptualized, critically revised and approved the final version of the manuscript; AT carried out data analysis and drafting of the manuscript; NI, NA and NO contributed to the surveillance activity and data collection.
References
Phase II was conducted from September 14, 2021 to November 19, 2021. By then, there were no local transmission cases, and positive cases were limited to only imported cases who had travelled into Brunei Darussalam from overseas. During this phase, a total of 190 companies were identified, and 10% of each company’s migrant workforce was selected for RT PCR testing. Out of 174 companies, 860 migrant workers were screened and tested negative. By then, Brunei had recorded 197 days of zero COVID-19 in local cases, and this may have been the probable reason for suboptimal participation of companies and migrant workers during this phase of active surveillance.
A different approach was adopted for phase III, which was conducted from March 22, 2021 to April 22, 2021. At this point, MOH had acquired a supply of COVID-19 antigen rapid test kits. This point of care testing was conducted at the Foreign Worker Health Screening Center, where migrant workers attended for their biennial health screening as part of their employment visa process.10 Every 5th migrant worker who attended the center was selected, which resulted in a total of 1510 migrant workers. Most of them were 30-40 years of age (35.8%) and men (68.3%). A similar distribution of the above nationalities was observed in this cohort; namely Indonesia (39.7%), Philippines (27%), Bangladesh (12%) and India (10.4%). Six of the workers were tested positive for SARS-CoV-2 antigen; however, according to the confirmatory RT PCR test done on the same day, all six results turned out to be negative.
Discussion
As SARS-CoV-2 does not discriminate against any individual, the migrant worker population is not spared from the virus. Their risk is often increased due to overcrowded living conditions, lack of accessibility to healthcare and hygiene practices, language and socio-cultural barriers.11,12 The World Health Organization (WHO) had published several guidance documents on COVID-19 surveillance in high risk populations. They included site-specific risk assessment and community-based surveillance as important strategies to prevent and contain rapid spread of the virus.11, 12 This paper described an active workplace surveillance for SARS-CoV-2, among migrant workers in Brunei Darussalam in a phased manner during the different stages of COVID-19 outbreak in the country. Phase I (April-June, 2020) of the surveillance was carried out when there was active community transmission, while phases II (September-November 2020) and III (March-April 2021) were conducted when there was no ongoing community transmission. Phase I identified three COVID-19 cases, that ultimately turned out to be the last three reported cases during Brunei’s first wave of outbreak. However, no positive cases were identified during phases II and III, which ensures the absence of any ongoing hidden transmission of disease. This low incidence can be attributed to an overall low level of infection during the first wave of COVID-19 in the country, i.e. a total of 141 cases reported from March 9, 2020 to May 6, 2020. This was followed by 196 imported cases entering Brunei from overseas by July 31, 2021. During the first wave, Brunei also recorded zero COVID-19 cases among healthcare workers, another high risk group identified for SARS-CoV-2 transmission globally.13 This successful control of pandemic was a result of strict public health measures adopted by MOH Brunei. It included restrictions of overseas travel and mass gatherings, increasing awareness and practices on hygiene measures and physical distancing, isolation/quarantine measures, as well as enforcing legislative provisions under the Infectious Disease Act of 2010. A test, trace and isolate approach and regular screening of high risk groups, such as healthcare workers and migrant workers, helped the nation to mitigate the threat of transmission of SARS-CoV-2.14, 15
Conclusion
Active COVID-19 screening of migrant workers in phase I during the time of ongoing community transmission, helped to detect three positive cases. They turned out to be the last reported local cases during the first wave of outbreak. Though the number of positive cases was small, this strategy actively searched for any positive cases among the registered migrant worker population in the country. Phases II and III of surveillance activities, further confirmed the absence of any hidden local transmission case in this population. Thus, a continuous phased and enhanced active surveillance strategy is beneficial not only in detecting local transmission cases that probably would have gone undetected, but also in confirming absence of any hidden ongoing transmission in this population. In addition, such data are useful to inform local authorities to take subsequent actions regarding further containment of COVID-19, and for collaborative efforts to be strengthened between the health sector and other relevant sectors responsible for health, safety and welfare of migrant workers in Brunei Darussalam.
Key Points for Enhanced Surveillance in Migrant Worker Population:
• Identifying high risk or vulnerable populations
• Developing or using an existing surveillance system to facilitate screening and testing in this population
• Collaborating with relevant organizations to facilitate surveillance
• Offering free surveillance screening and testing to migrant worker population
Conflict of Interest
None
Author's contributions
AL conceptualized, critically revised and approved the final version of the manuscript; AT carried out data analysis and drafting of the manuscript; NI, NA and NO contributed to the surveillance activity and data collection.
References
- International Labour Organization (ILO). International Labour Standards on Migrant workers. Available at https://www.ilo.org/ global/standards/subjects-covered-by-international-labour-standards/migrant-workers/lang--en/index.htm
- World Health Organization (WHO). COVID-19 immunization in refugees and migrants: principles and key considerations - Interim guidance. 2021. Available at https://apps.who.int/iris/ bitstream/ handle/10665/344793/WHO-2019-nCoV-immunization-refugees-and-migrants-2021.1-eng.pdf
- Hayward SE, Deal A, Cheng C, Orcutt M, Norredam M, Veizis A, et al. Impact of COVID-19 on migrant populations in high-income countries: a systematic review. European Journal of Public Health. 2021; 31 (Supplement 3). DOI: 10.1093/eurpub/ckab164.882
- Koh D. Migrant workers and COVID-19. Occupational and Environmental Medicine 2020; 77 (9): 634-6 DOI: 10.1136/oemed-2020-106626
- Ministry of Health. COVID-19 Situation report, 6 May 2020 Daily Report on COVID-19. Singapore. Available at https://www.moh. gov.sg/docs/librariesprovider5/2019-ncov/situation-report---6-may-2020.pdf
- World Bank Group. Potential Responses to the COVID-19 Outbreak in Support of Migrant Workers. 2020. Available at https://documents1. worldbank.org/curated/en/428451587390154689/pdf/Potential-Responses-to-the-COVID-19-Outbreak-in-Support-of-Migrant-Workers-June-19-2020.pdf
- International Labour Organization (ILO). Protecting migrant workers during the COVID-19 pandemic Recommendations for Policy-makers and Constituents, Policy brief. 2020. Available at https://www. ilo.org/wcmsp5/groups/public/---ed_protect/---protrav/---migrant/ documents/publication/wcms_743268.pdf
- Department of Economic Planning and Statistics Ministry of Finance and Economy Brunei Darussalam (DEPS-MOFE). Report of the Labour Force Survey 2020. Available at http://deps.gov.bn/DEPD %20Documents%20Library/DOS/Labour%20force%20survey_KTK/2020/RPT_2020.pdf
- Ministry of Health (MOH). Press release on the current situation of the COVID-19 infection in Brunei Darussalam. Brunei Darussalam, 2021. Available at http://www.moh.gov.bn/Lists/Latest%20news/ NewDispForm.aspx?ID=970019/KTK_2019.pdf
- Ministry of Health (MOH). Standard operating procedure for foreign workers’ health screening. Brunei Darussalam. 2016.
- World Health Organization (WHO). Promoting the health of Migrant Workers in the WHO European Region during COVID-19, 2020. Available at: https://apps.who.int/iris/bitstream/handle/ 10665/336549/WHO-EURO-2020-1384-41134-55925-eng.pdf?sequence=1&isAllowed=y
- The Lancet. COVID-19 will not leave behind refugees and migrants. The Lancet. 2020; 395 (10230): 1090.
- World Health Organization (WHO). Considerations for COVID-19 surveillance for vulnerable population, 2021 Available at: https://www.who.int/publications/i/item/considerations-for-covid-19-surveillance-for-vulnerable-populations
- Trivedi A, Fontelera M, Ishak N, Lai A, Win K, Ismail K et al. Healthcare workers’ preparedness and response during COVID-19 pandemic. Proceedings of Singapore Healthcare. 2021; 201010582110507.
- Wong J, Chaw L, Koh W, Alikhan M, Jamaludin S, Poh W et al. Epidemiological Investigation of the First 135 COVID-19 Cases in Brunei: Implications for Surveillance, Control, and Travel Restrictions. The American Journal of Tropical Medicine and Hygiene. 2020; 103 (4): 1608-1613.
Type of Study: Editorial |
Subject:
Special
Received: 2022/01/12 | Accepted: 2022/04/20 | Published: 2022/05/29
Received: 2022/01/12 | Accepted: 2022/04/20 | Published: 2022/05/29
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
